Earlier this week, the Herald had a story about antibiotics and childhood obesity. No-one involved really covers themselves in glory here, but probably the reporter comes out best.
The headline (Antibiotics ‘link to child obesity’) with appropriate claim quotes, and the lead
Children who are given antibiotics in the first two years of their lives are at greater risk of becoming obese in early childhood, a study suggests.
are fine, though there’s a sub-headline “Study finds some treatments kill bacteria that affect rate at which toddlers gain fat” that manages to be wrong in every respect.
The story goes on
The United States research is based on the medical records of 65,000 children between 2001-2013.
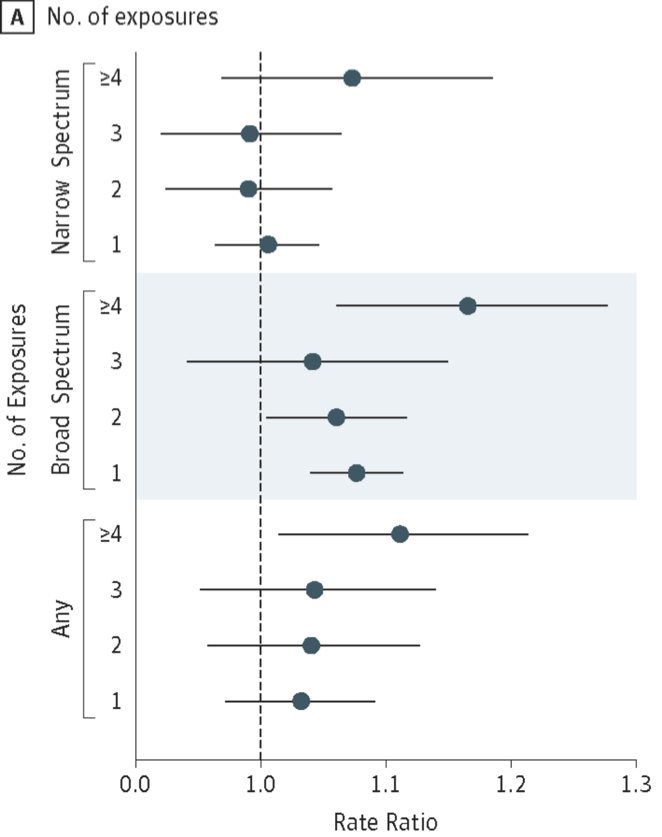
Researchers found infants who were given broad-spectrum antibiotics at least four times in their first two years were 16 per cent more likely to be obese by the age of 5.
That is in the research paper, but it’s much less impressive in context
The circles are the observed ratios of rates of obesity, the lines give the margin of error. You can see that, compared to no exposure, one exposure seems bad, two or three not so bad, and four or more worse. They’ve looked at a lot of comparisons that don’t show a clear pattern, and picked out the biggest number.
There are other quibbles, for example, ‘broad spectrum’ doesn’t mean what it usually means, it means ‘everything except penicillin and amoxicillin’, but the biggest problem is confounding. There are lots of things related to obesity and to antibiotic prescription, and it wouldn’t be at all surprising for one of them to explain this relationship.
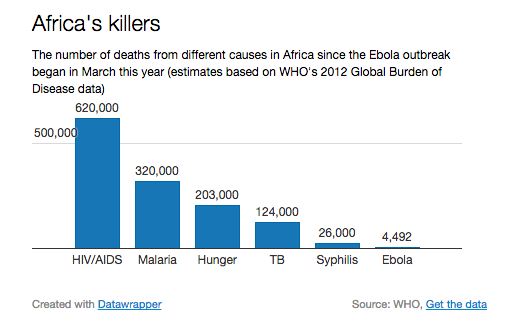
More importantly, there’s no way this explains any meaningful fraction of the increase in childhood obesity. Only about 3% of children were in the ‘4+ broad spectrum exposures’, so even if the ratio of 1.16 was true, the antibiotics would only be responsible for about half a percentage point of the obesity rate. Even less of the the obesity increase would be explained, since antibiotics aren’t actually completely new. Differences between countries also don’t seem to fit this as an explanation. For example, South Korea used to have a serious antibiotic overuse problem, which was reduced by new regulations in 2000. They don’t have much of a childhood obesity problem.
Still, there’s no reason the result couldn’t be true to some extent. Antibiotics do affect gut bacteria, and gut bacteria are important in metabolising food. It might be true, but it’s definitely being oversold, and there are more urgent reasons not to over-use broad spectrum antibiotics.
The other part of the story that’s disappointing for the light it casts on science communication is some of the response
Some New Zealand experts are sceptical. Fight the Obesity Epidemic founder Dr Robyn Toomath noted that the latest study was funded by the American Beverage Foundation for a Healthy America, founded by the soft-drink industry.
“This is the industry buying crap science,” she said. “People who are poor get sick and get more antibiotics. They are more likely to be fat and a lot of other things as well.”
I’m in favour of scientists commenting on public issues, and I don’t see anything wrong with advocacy, but I think public allegations of intellectual dishonesty need a bit more detailed backup than this. You’d almost get the impression that the research hadn’t looked at number of doctors visits or any indicators of poverty.