Dexamethasone and COVID
You’ve probably heard (Stuff*, NZ$ Herald) that there is a new treatment for serious cases of COVID-19, a drug called dexamethasone. There’s not a lot of controversy about the drug itself, but there’s some about the way the the announcement was handled and about the reporting.
Dexamethasone is a corticosteroid. Its main use is to shut down large chunks of your immune system. (The basic mechanism is the same as inhaled steroids for asthma and hay fever, but those are lower doses and are carefully engineered not to get into your blood stream, so they don’t have much effect outside your nose and lungs.) In serious cases of COVID, a patient’s immune system is extremely overactive, and clinical trials are looking at corticosteroids and at more selective ways to reduce immune activity.
Since fighting off viruses is part of the point of having an immune system, the drug is less likely to be helpful in less serious cases (and it didn’t show any benefit in people who weren’t on oxygen). It is extremely unlikely that dexamethasone would be helpful in preventing the disease — you’d expect it to increase risks. The tendency of the modern medical system to talk in terms of clinical evidence is bit of a problem here. People will say “there’s no evidence that it’s beneficial in prevention”, and a lay person can’t necessary tell where this is on the spectrum from “we don’t have clinical trial results yet so we’re being conservative” to “don’t inject bleach, it will kill you”.
So when the UK Secretary of State for Health poses in an ordinary chemist’s shop talking about community pharmacists and widespread availability of dexamethasone it’s not the best look.

What he would doubtless explain he means is that the UK government has made sure they have enough dexamethasone for the people who need it — but since there were 450,000 prescriptions for it in the year to March, it’s not exactly rare.
There’s a bit of disagreement in coverage about whether this is ‘low dose’ or ‘high dose’. That’s because dexamethasone is a very powerful corticosteroid, and it’s only used in settings where you really want the immune system to know what hit it. The 6mg/day dose is low or moderate for dexamethasone (compared to the doses used in some cancers) but it’s a high dose of steroid.
The actual controversy is about the results announcement. The researchers put out a press release saying that the trial had been stopped early because they were sure everyone should get dexamethasone, but there was very little data released. In this particular case no-one is suggesting that the data are completely made up or even that the specific numbers released are untrustworthy, but there is always an expectation that the researchers are putting their best foot forward in the press release. The final publication is often a bit less convincing, when all the measurements are taken into account.
Atul Gawande (well-known surgeon, writer, and public health researcher) said on Twitter
It will be great news if dexamethasone, a cheap steroid, really does cut deaths by 1/3 in ventilated patients with COVID19, but after all the retractions and walk backs, it is unacceptable to tout study results by press release without releasing the paper.
He’s got a point, but it’s not clear what the alternative was.
The Data Monitoring Committee (who get to see all the data) had recommended that the study stop randomly choosing people to not get dexamethasone. The trial management agreed. But the trial had been running all this time. There is more trial data on dexamethasone now than there was in the report to the Data Monitoring Committee, and the researchers need to redo the analysis with this extra data before they can publish a journal article (or even put out a preprint). The final results are not yet available.
On the other hand, the 173 hospitals participating in the trial need to know that they’re not randomising people to dexamethasone, and that it’s because it works, not because it doesn’t work. Even if none of them leak this information, new patients (and their families) will be given a different description of the possible treatments than previous patients received, and someone is going to notice. A press release is a lot better than the news just leaking out.
In some trials there is a partially mechanical set of plans for stopping and you could just put out a statement “blah blah met pre-specified stopping boundary blah blah further results soon”. But RECOVERY doesn’t have pre-specified stopping boundaries, because COVID treatment is such a fluid topic. Here, via Hilda Bastian, is the description
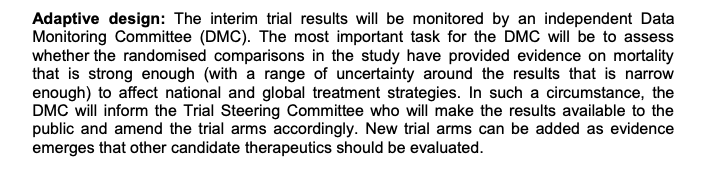
The Data Monitoring Committee are just supposed to use their best judgement as to whether the results will be convincing.
What I’d like to see in a situation like this is public release of the report to the Data Monitoring Committee, after any necessary redactions for privacy (eg, details of adverse events), and with big red flashing letters explaining that the final results will change slightly. But no-one should pretend this wouldn’t be revolutionary.
* I removed the Stuff link because the site autoplayed a video ad with the sound on.
Thomas Lumley (@tslumley) is Professor of Biostatistics at the University of Auckland. His research interests include semiparametric models, survey sampling, statistical computing, foundations of statistics, and whatever methodological problems his medical collaborators come up with. He also blogs at Biased and Inefficient See all posts by Thomas Lumley »