You can divide most of the coronavirus stories in the world media into two groups: accurate and helpful information on the one hand, and harmful misinformation on the other. The NZ media have been doing pretty well in keeping to the first sort.
There are a few stories in the middle, like this one at Newshub, that seem to be intended mostly as entertainment
Some people are making sure they will enjoy their time in quarantine, should it be enforced upon us.
New Zealand sex retailer Adult Toy Megastore has reported a surge of sales in lubricant, vibrators and batteries in the wake of the pandemic.
They don’t sell toilet paper or bottled water, so they’re bound to have somewhat different top products from the supermarkets, and there’s nothing really surprising here. In contrast to the previous StatsChat appearances of this store, they’re sticking to topics where they actually know the data, rather than overinterpreting bogus surveys.
There’s also a pointer to some medical advice, which is where the whole thing gets a bit more dodgy. The only reason I’m keeping this to “a bit” is that I don’t think you’re intended to really take the story seriously:
“Masturbation can produce the right environment for a strengthened immune system,” she told Men’s Health.
Her views are backed up by a study from the Department of Medical Psychology at the University Clinic of Essen which looked at the effects of orgasm through masturbation on the white blood cell count.
A group of 11 volunteers were asked to participate in a study and the results confirmed that sexual arousal and orgasm increased the number of white blood cells.
The study is actually linked. It’s a paywalled paper, but here’s the abstract.
If you’ve got an experimental study of an intervention that might prevent viral infection, you’d want to know who was being studied, the sample size, and how representative they were. You’d want to know what effects were being measured and over what period. And you’d want to know to what extent the intervention was also present in the control group. In a serious clinical trial that sort of information would be in the abstract.
The abstract doesn’t actually say anything about the diversity of study population, apart from “11 volunteers”. The paper says “healthy young males” and notes they were all exclusively heterosexual and had an average age of 37.7 (so ‘young’ is being interpreted relatively broadly). The participants were asked to refrain from sexual activity for 24 hours before the experiment, but that’s all.
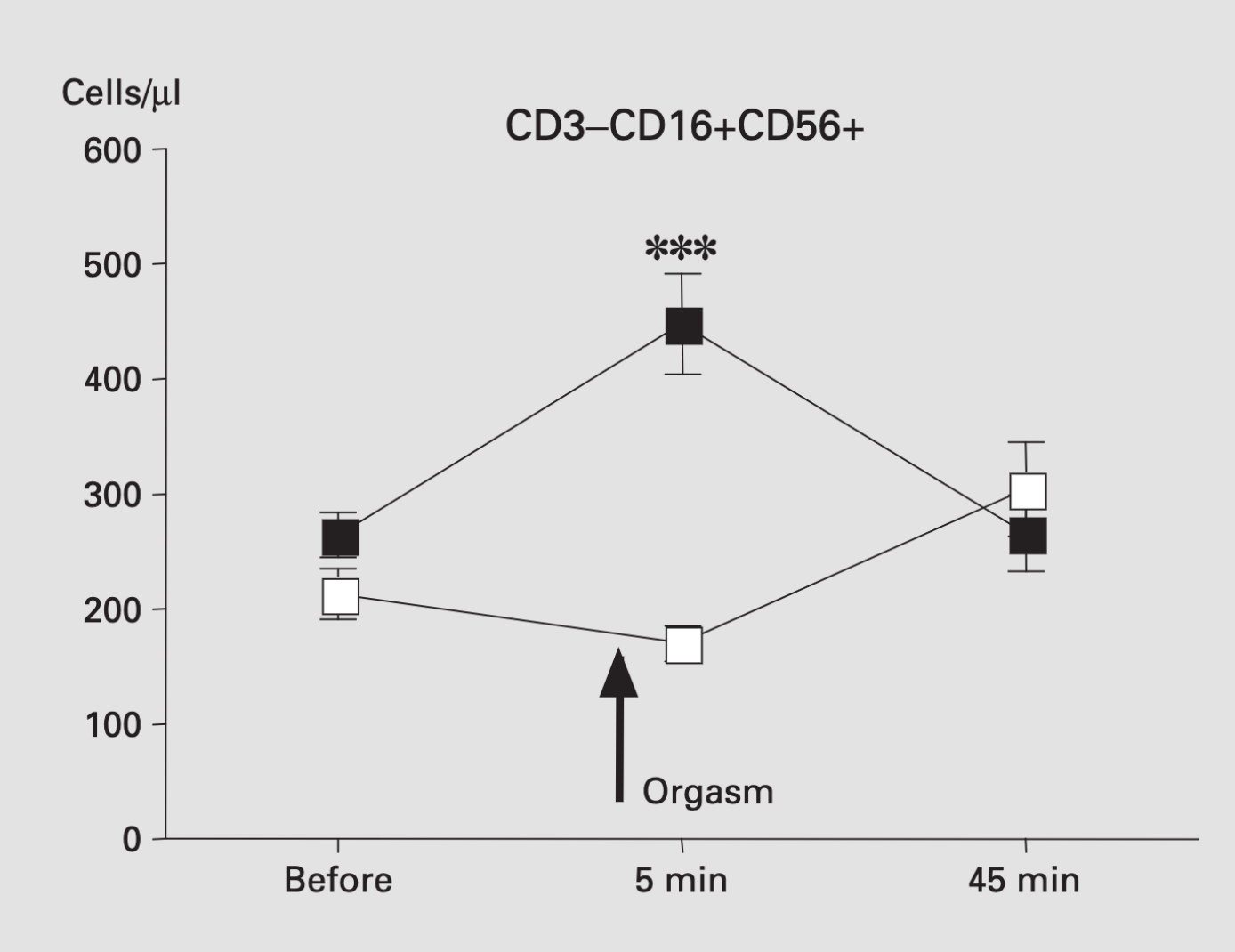
The abstract does talk, importantly, about “transient” changes in hormones. It’s less open about the changes in white blood cells. The headline effect is that there were more “NK cells“, which are theoretically relevant to viral infection, 5 minutes after orgasm. It’s not clear whether the increase is big enough to be helpful. However, the increase had gone away again by the second measurement at 45 minutes (so it’s probably safe). Here’s the graph
It’s not clear that we should believe these results, given the well-known problems with reporting and analysis bias in small experiment — and even without any issues in the scientific publication process, you can be pretty confident Newshub wouldn’t have mentioned unconfirmed results from a tiny experiment published in 2004 if it didn’t confirm what they wanted to say. But suppose we do believe the results. What does it tell us about COVID-19? Is this, as they say, news you can use? You might consider your times of greatest exposure to other people’s viruses and look for a half-hour window where greater immunity would be relevant. On the other hand, that might cause more problems than it solves. Alternatively, you could just wash your hands (actually, you should wash them either way).
Leaving aside the questions of appropriate time and place, I think the StatsChat advice on red wine and chocolate also applies here. If you’re thinking of a half-hour increase in one type of white blood cells as a convincing argument in favour of orgasms, you may be doing them wrong.