May 7, 2013
Video on randomised trials — in poverty relief
The organisation Innovations for Poverty Action have made a neat little animated video explaining how and why they do randomised controlled trials of poverty-relief programs.
The organisation Innovations for Poverty Action have made a neat little animated video explaining how and why they do randomised controlled trials of poverty-relief programs.
From a comment piece in Stuff, by Bruce Robertson (of Hospitality NZ)
In the past five years, the level of hazardous drinking has significantly decreased for men (from 30 per cent to 26 per cent) and marginally decreased for women (13 per cent to 12 per cent).
There was a modest but important drop in the rates of hazardous drinking among Maori adults, with the rate falling from 33 per cent to 29 per cent in the latest survey.
As @tui_talk pointed out on Twitter, that’s a four percentage point decrease described as “significant” for men and “modest” for Maori.
At first I thought this might be a confusion of “statistically significant” with “significant”, with the decrease in men being statistically significant but the difference in Maori not, but in fact the MoH report being referenced says (p4)
As a percentage of all Māori adults, hazardous drinking patterns significantly decreased from 2006/07 (33%) to 2011/12 (29%).
StatsChat spends a lot of time criticizing bad graphs. Here’s a simple but good graph, from the Calculated Risk blog
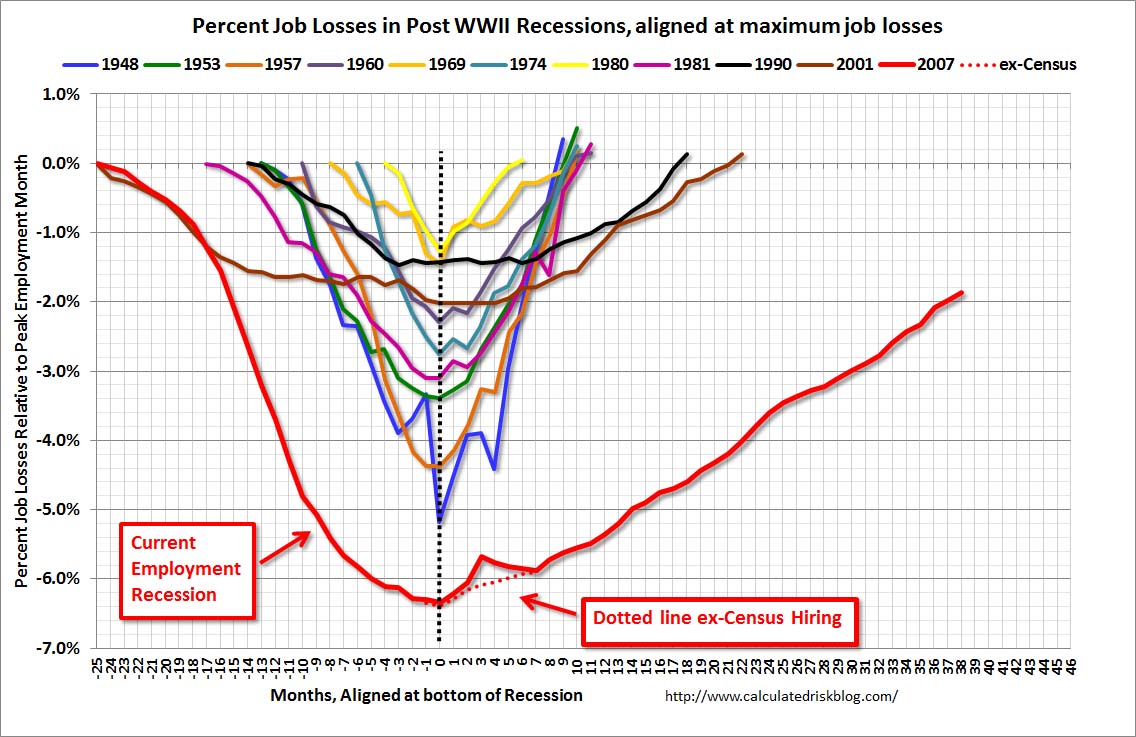
The graph shows employment during US recessions, aligned at the point of maximum job loss. It clearly demonstrates that the current Great Recession is very different from all the other post-WWII recessions, both in depth and in duration.
It would be easy to quibble with some design choices in the graph, but it fulfills the basic requirements admirably: the real difference is visually dramatic, and it wouldn’t be visually dramatic if it weren’t real.
As I’ve commented before, it’s hard to find examples of the drafting and redrafting process for graphics, which is just as necessary as it is for text.
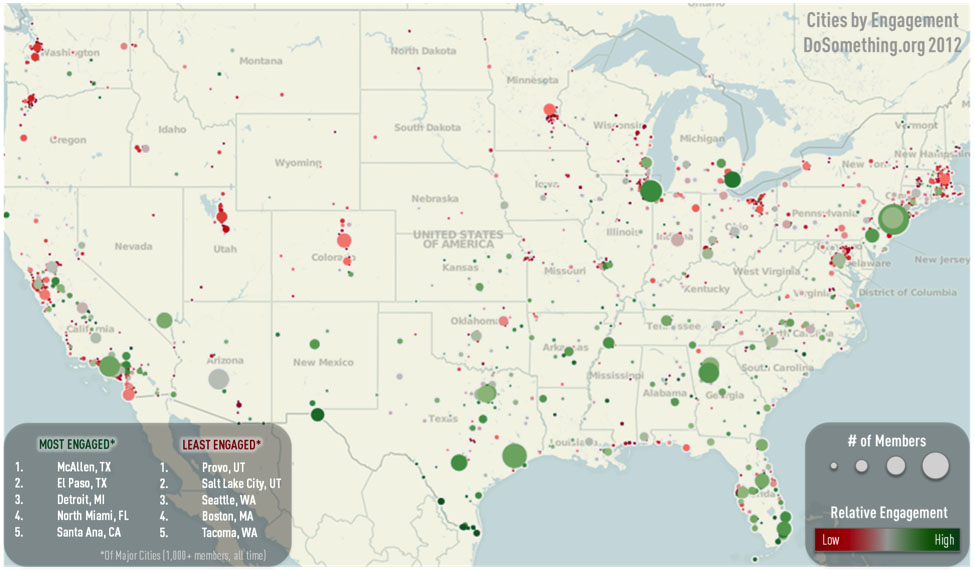
A post at Harvard Business Review describes the process, in the setting of a large non-profit organisation, with this as the result
The `pie’ in pie-chart is a metaphor — the charts are divided into slices in the way that certain kinds of pie are, and the slices add up to the whole pie.
Or, at least, that’s usually the idea. One of StatChats’s foreign correspondents sent in this effort from the BBC
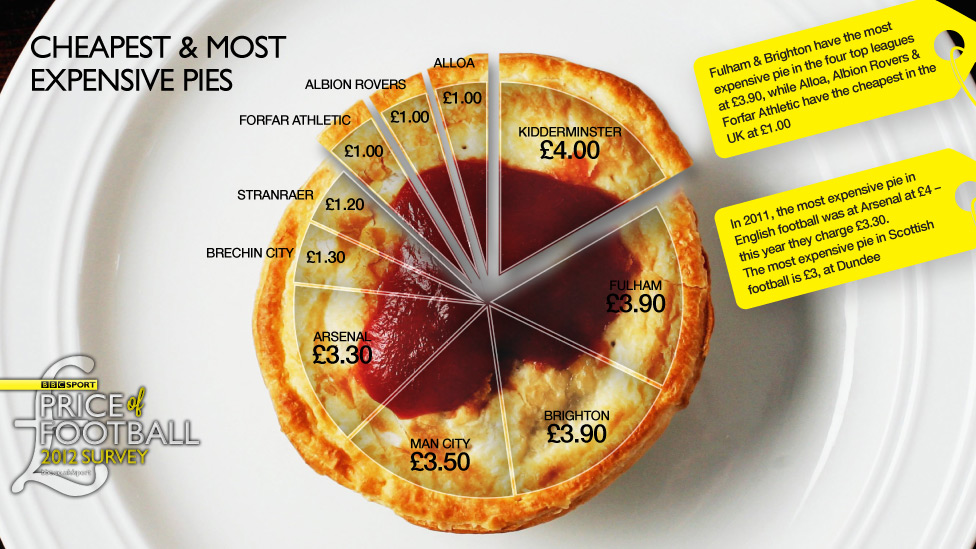
This kind of pie doesn’t get divided into slices — it would just fall apart. And in this graph the slices don’t add up to anything meaningful — for those of you not up on the British sports scene: there are actually more than ten football clubs. In the graphic we have Premier League teams such as Arsenal and Manchester City mixed in with Albion Rovers and Brechin City from the Scottish 2nd division.
The pie price pie exemplifies a general rule, if you have to write all the data values on your graph, the graph isn’t doing its share of the work.
Each week, we would like to invite readers of Stats Chat to submit nominations for our Stat of the Week competition and be in with the chance to win an iTunes voucher.
Here’s how it works:
Next Monday at midday we’ll announce the winner of this week’s Stat of the Week competition, and start a new one.
If you’d like to comment on or debate any of this week’s Stat of the Week nominations, please do so below!
Stuff has a story (borrowed from the West Island) headlined “Over 40? Five tests you need right now”.
You might have expected some reference to the other recent news about screening: that the US Preventive Services Taskforce has now joined the Centers for Disease Control in recommending universal screening for HIV (as TVNZ reported). It’s not clear if New Zealand will follow the trend — HIV infection in people not in high risk groups is less common here than in the US, so the benefit compared to more selective screening is smaller here. This illustrates the complexities of population screening. Not only does the test have to be accurate, especially in terms of its false positive rate, but there needs to be something useful you can do about a positive result, and screening everyone has to be better than just screening selected people.
So, let’s compare the suggestions from Stuff’s story to what national and international expert guidelines say you need.
Two of the tests, for high blood pressure and high cholesterol, are spot on. These are part of the national 2012/13 Health Targets for DHBs, with the goal being 75% of the eligible population having the tests within a five-year period. The Health Target also includes blood glucose measurement to diagnose diabetes, which the story doesn’t mention. The US Preventive Services Taskforce also recommends blood pressure and cholesterol tests, though it recommends universal diabetes screening only after age 50 or in people with high blood pressure or people with risk factors for diabetes.
One of the tests recommended in the story is a depression/anxiety questionnaire, for diagnosing suicide risk. Just a couple of weeks ago, the US Preventive Services Taskforce issued guidelines on universal screening for suicide prevention by GPs, saying that there wasn’t good enough evidence to recommend either for or against. As the coverage from Reuters explains, these questionnaires do probably identify people at higher risk of suicide, but it wasn’t clear how much benefit came from identifying them. So, that’s not an unreasonable test to recommend, but it would have been better to indicate that it was controversial.
One more of the tests isn’t a screening test at all — the story recommends that you make sure you know what a standard drink of alcohol is.
The top recommendation in the story, though, is coronary calcium screening. The US Preventive Services Taskforce recommends against coronary calcium screening for people at low risk of heart disease and says there isn’t enough evidence to recommending for or against in people at higher risk for other reasons. The American Heart Association also recommends against routine coronary calcium screening (they say it might be useful as a tiebreaker in people known to be at intermediate risk of heart disease based on other factors). No-one doubts that calcium in the walls of your coronary arteries is predictive of heart disease, but people with high levels of coronary calcium tend to also be overweight or smokers, or have high blood pressure or high cholesterol or diabetes — and if they don’t have these other risk factors it’s not clear that anything can be done to help them.
As an afterthought on the coronary calcium screening point, the story has an additional quote from a doctor recommending coronary angiography before starting a serious exercise program. I’d never heard of coronary angiography as a general screening recommendation — it’s a bit more invasive and higher-risk than most population screening. It turns out that the American College of Cardiology and the American Heart Association are similarly unenthusiastic, with their guidelines on use specifically recommending against angiography for screening of people without symptoms of coronary artery disease.